


Vaccine Surveillance Report or ‘Vaccine’ Surveillance Report?
Vaccine Surveillance Report or ‘Vaccine’ Surveillance Report?
This article was published by Holding the Line: Journalists Against Covid Censorship:
https://holding-the-line.com/2021/11/12/vaccine-surveillance-report-or-vaccine-surveillance-report/
This article will be posted twice - the second time with a different title to make it more Twitter friendly. There is a fair chance that the Big Tech totalitarian fact-checking algorithms will be unamused when they detect the sacred V word in quote marks. This could be viewed as blaspheming the Covid cult. So, the second time it pops into your inbox it will be titled "Defending the Indefensible".

Before looking at a headline summary of Covid hospitalisation and death data included in the UK Health Security Agency’s (UKHSA) Vaccine Surveillance Report for week 44, it is important to remind ourselves of the shakiness of one of the pillars that is foundational to much of the data in this report – testing and cases.
In ‘case’ of emergency press pause
After an 18-month onslaught of a mass testing regime, it’s easy to forget that the mass testing paradigm is a flawed one, especially when it is embedded in so much of the reporting that the Government desperately uses to try to get us to believe in the official Covid narrative. So perhaps we should remind ourselves that reliable independent media sources have reported extensively on the inaccuracy of both the PCR test – the linked expert analysis suggests mass testing leads to as many as 99% of positive results being false – and lateral flow test.
Yes, the above link to the critical analysis of PCR test’s reliability is over a year old but what has changed since then to transform it into a beacon of light in diagnostic testing? It is still the same test whose inventor said should not be used as a diagnostic tool let alone a mass screening tool. Its unfitness for purpose has been underscored by a Portuguese Courtwhich ruled, based on expert testimony, that the ‘the PCR process is not a reliable test for Sars-Cov-2’ and cited a study that pointed to potentially 97% of positive results being false positives when running the test at 35 cycles or more.
Apart from being phenomenally unreliable, Covid testing has been hugely successful in propagating a wider insidious process of normalising the abnormal by an attempted nullification of the fundamental medical tenet that a ‘case’ is both symptomatic and must be diagnosed by a doctor. Research shows that 86% of people who test positive have no symptoms at all. So, 86% of people who test positive for Covid would not know they have Covid in the absence of a test, which says a lot about the apocalyptic hype that has surrounded this virus. Considering the test’s unreliability and absence of symptoms in 86% of test results, is it too presumptuous to ask if the 86% actually have Covid?
As with much politicised science in the Covid era, the study’s finding is turned on its head – rather than challenge the meaning and reliability of the test, the authors call for “more widespread testing…to catch ‘silent’ transmission.”
Using the 86% non-symptomatic test statistic as a guideline, it’s easy to see how the UKHSA’s alarming week 44 report of 975,224 cases in weeks 40-43 is actually not that alarming since 838,692 were probably oblivious of their ‘condition’ right up to the moment they were told there was something ‘wrong’ with them. The vast gap between 975,224 ‘cases’ and people needing treatment in hospital (8,637 or 0.9% of the total cases) tends to give some credence to the claim that the majority of those testing positive are false positives.
Moreover, a staggering 11.1m tests were conducted across the UK in weeks 40-43 to generate these cases. The cost of the Government’s NHS Test and Trace program according to the parliamentary Public Accounts Committee (PAC) is £37bn. So, you’ve got to ask: what is it all for? Has it made a positive change? The PAC answered that question with its report card: “despite the unimaginable resources thrown at this project Test and Trace cannot point to a measurable difference to the progress of the pandemic”.
Following this damning indictment, it would be rational of you to think that the PAC’s recommendation would be to turn off the taxpayer money hose and bring the whole scandal of meaningless testing to an abrupt halt. But such rationality would demonstrate a misunderstanding of how Covid logic and Covid economics works. Like much Covid science, the PAC turned its report finding on its head by telling the Government to make the unworkable workable, instructing it to “rapidly turn around these fortunes and begin to demonstrate the worth and value of this staggering investment of taxpayers' money”!
Sane members of the public scratch their heads while the £1000 per day consultants that the PAC lambasts in its report breathe a sigh of relief.
To the extent that case numbers mean anything, they appear to demonstrate, on the Government’s own terms (namely the use of the mass testing juggernaut), that the vaccines are not just useless at preventing infection and transmission, but that they appear to enhance infection and transmission in the 40-79 age group, based on data in the week 43 report. Yes, you read that correctly. The vaccines register negative efficacy rates in this age group which means, if you are over 40, you are twice as likely to get infected after receiving the jab than if you had opted out of the biggest experiment ever conducted in the history of experimentation on humans, or possibly any life form including lab rats.
I think it’s safe to say this is precisely the sort of occurrence that was uppermost in the mind of the person who coined the expression: ‘sobering thought’. Following a reprimand from the U.K. Statistics Authority, the UKHSA has denounced the use of its unadjusted numbers to calculate vaccine efficacy and its arguments have been countered by those doing the analysis of vaccine efficacy that the Government refuses to do. We fully support the right of journalists to responsibly analyse and comment on data produced by the Government to allow the public to make up their own minds.
For all the above reasons, I have not analysed the week 44 case data and, in a sense, the headline commentary on cases has now been made.
Deaths within 60 days of a positive Covid-19 test
The table below is a summary of deaths within 60 days of a positive Covid-19 test for weeks 40-43, excluding unlinked* cases which are those where NHS numbers were unavailable to link to the National Immunisation Management System database. Unlinked deaths totalled 19 or 0.5% of the total number reported.

The same data presented graphically looks like this:
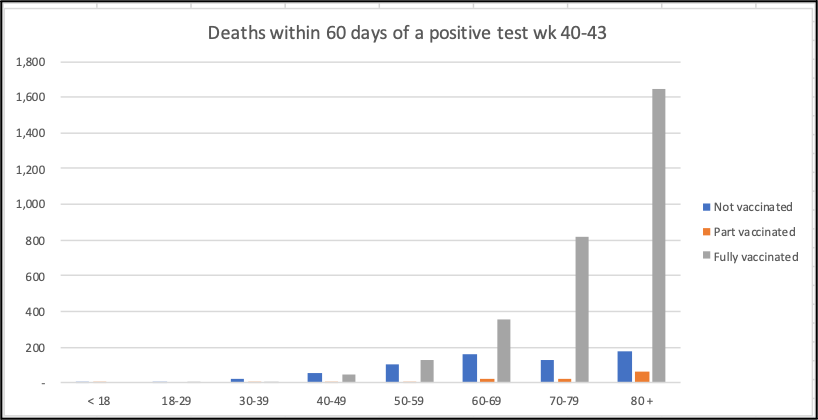
Because all deaths included in these figures are those that occurred within 60 days of a positive test result, the proportion for which Covid was determined to be the primary cause of death is not known.
Total linked deaths within 60 days of a positive Covid-19 test over the four-week period amounted to 3,804. Total deaths registered in England and Wales from all causes in the comparable four-week period were 44,279. Covid associated deaths comprise 9% of that total (6% for weeks 39-42).
79% of all Covid associated deaths were in the fully vaccinated (79% for weeks 39-42).
According to the NHS Covid-19 Vaccination Statistics for England for the week ending 31 October 2021, 85.4% of individuals aged 18 and over have been vaccinated with two doses.
Less than 3% of under 18s have received a second dose as of 31 October.
75% of all linked deaths in weeks 40-43 occurred in those aged 70 years and over (77% for weeks 39-42).
Hospitalisation
The table below is a summary of the hospitalisation numbers excluding unlinked cases* which totalled 85 or 0.97%% of the total number reported.
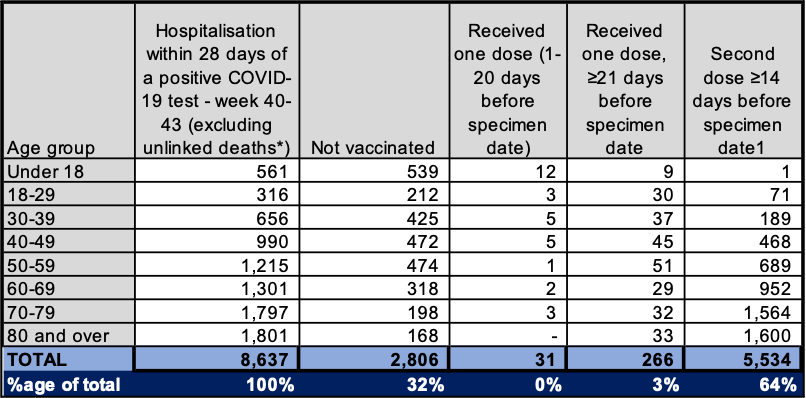
64% of all hospitalisations are in the unvaccinated. This rises to 69% if you exclude the under 18 age group which, according to the NHS Covid-19 Vaccination Statistics for England, is under 3% fully vaccinated as of 31 October.
The UKHSA Vaccine Surveillance report for week 44 states that: “By 31 October 2021, the overall vaccine uptake in England for dose 1 was 66.4% and for dose 2 was 60.9%.”
In closing
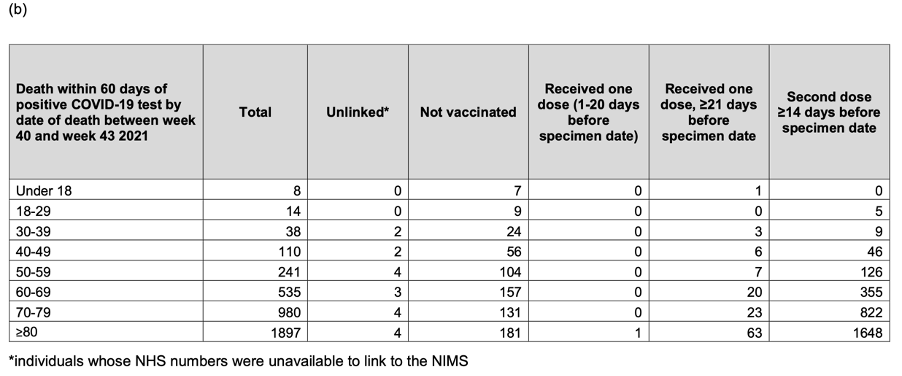
The week 44 Vaccine surveillance report, under the heading “Results” on page 14, claims that: “The rate of death within 28 days or within 60 days of a positive COVID-19 test increases with age, and again is substantially greater in unvaccinated individuals compared to fully vaccinated individuals.” [emphasis added]
I find it hard to reconcile the last part of that statement with the table and graph above that are derived from the data in the same UKHSA report on page 19. For the avoidance of doubt, here is a screen grab of the report’s death numbers which you may add up for yourself:
On 4th November, BMJ editor Dr Peter Doshi gave evidence at an expert panel on Covid vaccines held by Senator Ron Johnson in Washington DC. Challenging the ‘conventional wisdom’ that the clinical trials had proved that the vaccines saved lives, he had this to say:
“But is it true? When that statement by prominent public health officials was penned, there had been just one death, one death across the 70,000 Pfizer and Moderna trial participants. Today, we have more data, and you can see that there were similar numbers of deaths in the vaccine and placebo groups. The trials did not show a reduction in death. Even for Covid deaths, as opposed to other causes, the evidence is flimsy, with just two deaths in the placebo group versus one in the vaccine group. My point is not that I know the truth about what the vaccine can and cannot do, my point is that those who claimed the trials showed the vaccines were highly effective in saving lives were wrong. The trials did not demonstrate this.” [Emphasis added]
He also had this to say about the vaccines, or ‘vaccines’ if you are inclined to share Dr Doshi’s eloquently expressed doubts about the classification of Big Pharma’s new treatments as vaccines or if you question the CDC’s redefining of what a vaccine is:
‘I am one of the academics that argues that these mRNA products, which everybody calls vaccines, are qualitatively different than standard vaccines. And so I found it fascinating to learn that Merriam-Webster changed its definition of “vaccine” early this year. mRNA products did not meet the definition of “vaccine” that has been in place for 15 years in Merriam-Webster, but the definition was expanded such that mRNA products are now vaccines. I highlight this to ask a question: How would you feel about mandating COVID vaccines if we didn’t call them vaccines? What if these injections were called “drugs” instead? So here’s the scenario: We have this “drug”, and we have evidence that it doesn’t prevent infection, nor does it stop viral transmission, but the “drug” is understood to reduce your risk of getting very sick and dying of COVID. Would you take a dose of this drug every six months or so for possibly the rest of your life if that’s what it took for the drug to stay effective? Would you not just take this drug yourself, but support regulations mandating that everybody else around you take this drug? Or would you say, “Hold on a sec”. Maybe you’d say that, “If that’s all the drug does, why not use a normal medicine instead? The kind we take when we’re sick and want to get better? And why would you mandate it?”
He punctuated the end of his presentation with this observation: ‘I think it’s time to inject some critical thinking into that conversation [about the vaccines and mandates] and that is what I hope we are doing today.’
Dr Doshi is very old-fashioned indeed.